

12 Apr Understanding Frozen Shoulder

Have you ever felt the excruciating pain of a frozen shoulder? It is a very frustrating condition and can be very confusing to understand what it is and how to treat it. I would like to shed some light on this, or rather, hack at it with an ice pick for some better understanding. Curl up with your laptop and enjoy some dense reading…
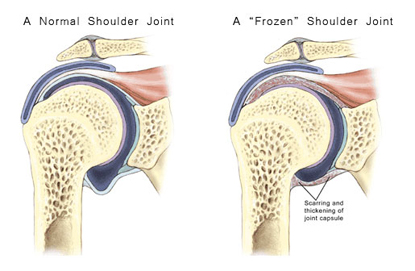
Adhesive Capsulitis, or frozen shoulder, is a painful condition that results in a severe loss of motion in the shoulder. It may follow an injury to the shoulder, but may also arise gradually with no warning or injury. Intermittent periods of use may cause inflammation and adhesions to grow between the joint surfaces, thus restricting motion. There is also a lack of synovial fluid to lubricate the gap between the arm bone and socket that normally helps the shoulder joint to move. This restricted space between the capsule and ball of the humerus distinguishes adhesive capsulitis from the less complicated condition known as stiff shoulder.
Anatomy
The shoulder is made up of three bones: the scapula (shoulder blade), the humerus (upper arm bone) and the clavicle (collarbone). The shoulder joint capsule is a loose bag of tissue that completely surrounds the shoulder joint. The joint capsule is made up of ligaments that form this watertight bag. A ligament is a soft tissue structure made up of connective tissue. Ligaments attach bones to bones. Inside the bag there is a small amount of joint fluid that lubricates the joint surfaces. This bag that makes up the joint capsule has a considerable amount of slack, loose tissue, so that the shoulder is unrestricted as it moves through its rather large range of motion.
Causes
The cause of this condition is largely a mystery. One theory is that the condition may be due to an autoimmune reaction. During an autoimmune reaction the body’s defense system that normally protects it from infection, mistakenly begins to attack parts of the body itself. The body thinks that the tissue it is attacking is foreign material. This causes an intense inflammatory reaction to the tissue that is under attack. The shoulder actually “freezes up” due to the severe inflammation of the joint capsule. The loose tissue of the joint capsule that usually allows a great deal of motion at the shoulder sticks together, limiting the motion. Why this should occur all of a sudden is a mystery.
Adhesive capsulitis may begin following other injuries where the shoulder is not moved around normally because of the other injury. A common example is after a wrist fracture, where the arm may be kept in a sling for several weeks. For some reason, this seems to start the process in some people. The condition has also been known to occur after surgical procedures for something unrelated to the shoulder and even after recovering from a heart attack.
The condition can begin while other shoulder problems are present. Sometimes, problems such as bursitis, impingement syndrome, or a partial rotator cuff tear can lead to a frozen shoulder as well. The pain from the first condition may cause you to decrease the use of the shoulder, and the underlying condition itself may lead to chronic inflammation. These two things combine to make a dangerous situation to develop adhesive capsulitis. Usually, the adhesive capsulitis must be treated first to regain motion in the shoulder before the underlying problem can be addressed.
Symptoms
The symptoms are primarily pain and a very reduced range of motion in the joint. The range of motion is the same whether your are trying to move the shoulder under your own power or if someone else is trying to raise the arm for you. There comes a point in each direction of movement where the motion simply stops as if there is something blocking the movement. The shoulder usually hurts when movement reaches the limit of the range of motion, and can be quite painful at night.
Diagnosis
The diagnosis of adhesive capsulitis is usually made on the history and physical examination. One key finding that can help differentiate adhesive capsulitis from a rotator cuff tear is how the shoulder moves. In adhesive capsulitis the shoulder motion is the same, whether the patient or the doctor tries to move the arm. In a rotator cuff tear, the patient cannot move the arm, but when someone else lifts the arm it can be moved in a nearly normal range of motion. X-rays are usually not helpful. An arthrogram may show that the shoulder capsule is scarred and contracted. This test is done by injecting dye into the shoulder joint and taking several X-rays. When this is done in the shoulder with adhesive capsulitis the first thing the radiologist will notice is that not much dye can be injected into the shoulder joint – the capsule of the joint is contracted and, thus, smaller than normal. The X-rays taken after injecting the dye will show very little dye in the joint.
As the motion increases in the shoulder, your doctor may suggest tests that look for an underlying condition, such as impingement, or a rotator cuff tear that may have initiated the condition. Probably the most common test used is the MRI scan. A MRI scan is a special radiological test where magnetic waves are used to create pictures that look like slices of the shoulder. The MRI scan shows more than the bones of the shoulder. It can show the tendons as well, and whether there has been a tear in those tendons.
Treatment
Treatment of the frozen shoulder can be frustrating and slow. Most cases will eventually improve, but it may be a process that takes months. Initial treatment is directed at decreasing inflammation and increasing the range of motion of the shoulder with a stretching program. Anti-inflammatory medications may be prescribed. It is critical that a Physical Therapy program be started and continued to regain the loss of motion.
An injection of cortisone and long-acting anesthetic, similar to novocaine, may bring the inflammation under better control, and allow the stretching program to be more effective. In some cases, injecting a long acting anesthetic along with the cortisone right before a stretching session with the Physical Therapist can allow the therapist to break up the adhesions while the shoulder is numb from the anesthetic.
If progress is slow, your doctor may recommend a manipulation of the shoulder while you are under anesthesia. This procedure allows your doctor to stretch the shoulder joint capsule, and break up the scar tissue while you are asleep. In most cases, a manipulation of the shoulder will increase the motion in the shoulder joint faster than allowing nature to take its course. It may be necessary to repeat this procedure several times.
Sorry, the comment form is closed at this time.